Here‘s what you can do with Landing Kit today
Create entire microsites using any selection of published resources
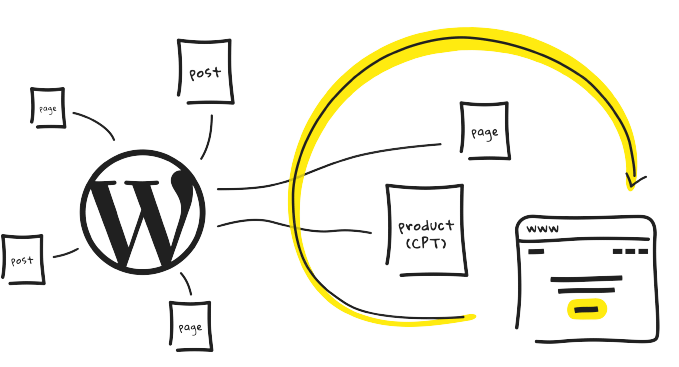
Landing Kit enables you to create landing pages or complete microsites by mapping domains and domain URL’s to any published resource within WordPress without the need for separate WordPress installations or a multisite install effectively turning your single WordPress installation into an unlimited landing page powerhouse.
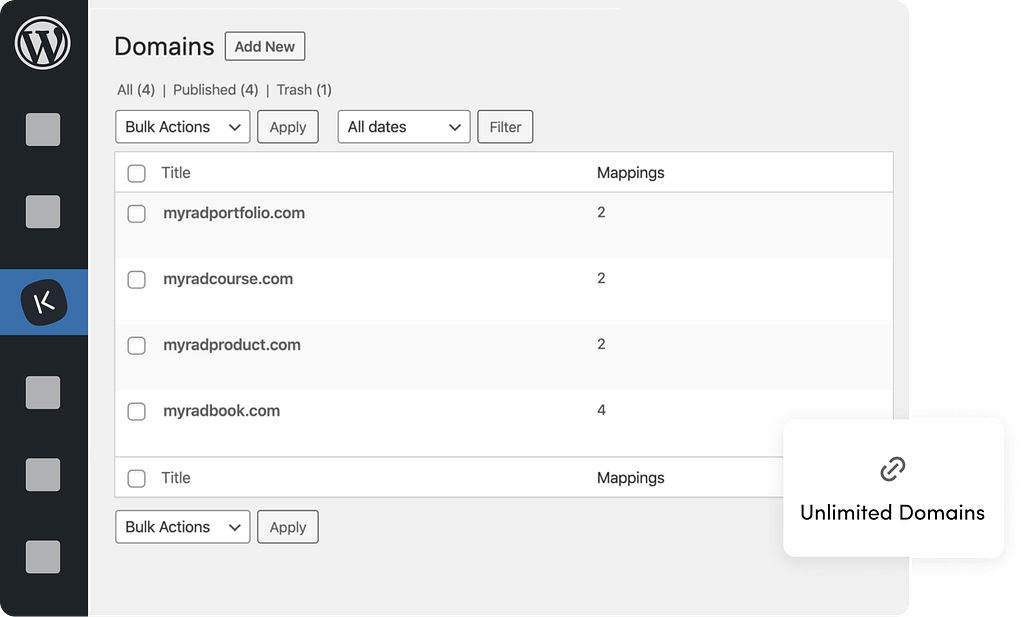
Unlimited domain
There’s no limit to how many domains you can use with a single WordPress install using Landing Kit. You can map as many domains as there are published posts, pages, or any other published custom post type entry.
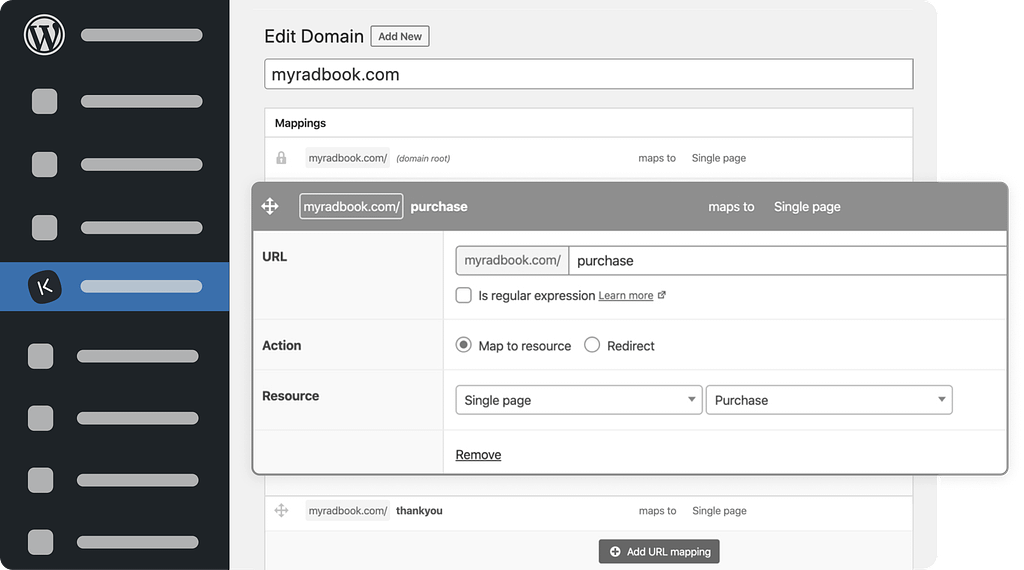
Subpage support
You’re not limited to single-page websites with Landing Kit… create complete microsites by mapping domains and domain URL’s to any published resource within WordPress.
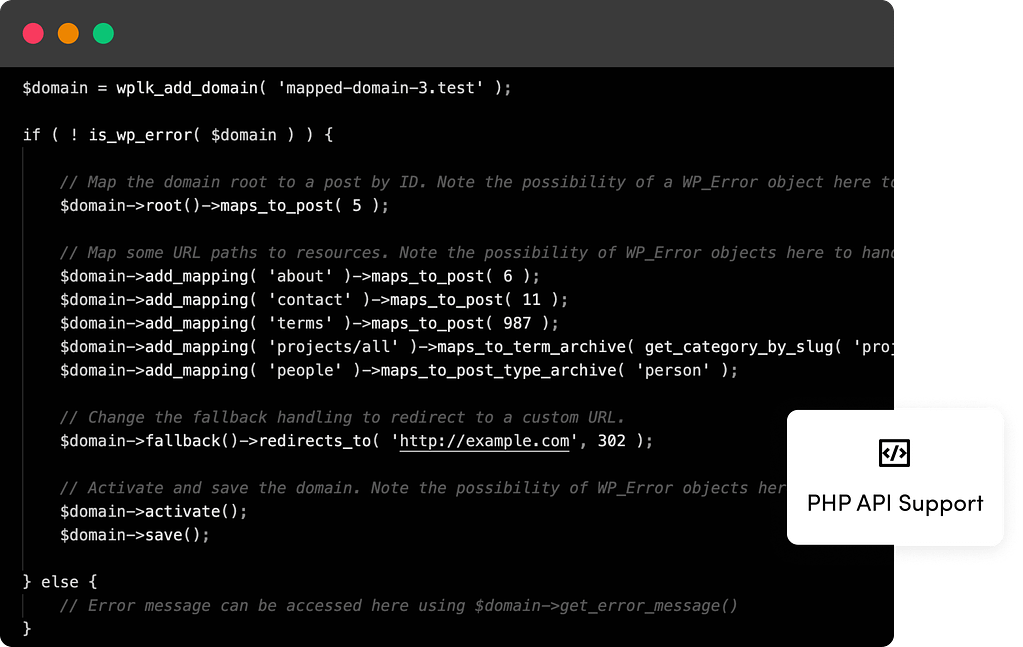
Oh hey, we have tools for developers too! Check out our PHP API
Landing Kit doesn’t end with mapping domains … we’ve launched a simple PHP API that enables developers to programmatically work with domains.
Our Users Love WP Landing Kit
I highly recommend WP Landing Kit to anyone who would benefit from mapping additional domain(s) to pages / post on an existing website(s). It’s simple, elegant and might be exactly what you need.

The product works like a charm!!! Simply magical!!! Now my only concern is trying to effectively choose when to use multisite and when to use Landing Kit.

I have tried the multiple domain mapping plugin previously but was not able to set it up properly/ make it work. The documentation and how this WP Landing Kit works is very straightforward, easy to follow & set up.

Find The Right Plan For You
- Support & Updates for 1 site
- Post Type Support
- WooCommerce Product Support
- Subpage Support
- Unlimited Domains
- Redirect Options
- SSL Enforcement
- PHP API
- Support & Updates for 5 sites
- Post Type Support
- WooCommerce Product Support
- Subpage Support
- Unlimited Domains
- Redirect Options
- SSL Enforcement
- PHP API
- Support & Updates for unlimited sites
- Post Type Support
- WooCommerce Product Support
- Subpage Support
- Unlimited Domains
- Redirect Options
- SSL Enforcement
- PHP API

100% Money-Back Guarantee!
Purchase with peace of mind. If you find out that this plugin does not meet your needs, we offer a 30-day no-questions-asked money-back guarantee. You can change plans or cancel your account at any time!
Supported by Real People
ThemeIsle is a global remote team of passionate WordPress professionals delivering awesome themes and plugins for more than 471,039 users.

Our products be used by
TOP NOTCH SUPPORT
Need support? Stay relaxed,
we have you covered!
Our Happiness Engineers are happy to help you get the best results from our products. No matter the question, we deal with it and don’t leave you wondering what to do.
- Large Knowledge Base
- 300+ Product Docs
- 200+ Video Tutorials
- Support via Email
- 1 Business Day Reply
- Priority Support
NEED A HAND?
Frequently Asked
Questions
In short, you need hosting with the ability to add alias or addon domains, a static IP address, and the latest version WordPress.
You should be familiar with:
- WordPress and the WordPress admin.
- Installing and activating plugins within WordPress.
- Adding alias or addon domains withing your WordPress host.
- Managing DNS records for your domain names. Specifically, you’ll need to be able to add/manage A-Records.
Everything you need to get started with Landing Kit can be found in the documentation.
Landing Kit is 100% compatible with all post, page and custom post type entries, including those created with the new Gutenberg editor.
By default, if a post has a mapped domain, the post can be accessible on both the mapped domain and the original URL. We have a 301 redirect options you can use to redirect the original post URL to the mapped domain.
There’s no limit to how many domains you can use with a single WordPress install using Landing Kit. You can map as many domains as there are published posts, pages or any other published custom post type entry.
If you have not found the answer to your question here, get in touch and we will be happy to help.